Swine Flu Influenza Type A/H1N1 Protection for Health Care Practitioners and Their Patients
14 years, 8 months ago
17816
0
Posted on Aug 13, 2009, 6 p.m.
By Gordon Pedersen Ph.D.
H1N1 is a serious threat to our health and way of life. The best way to treat it influenza is to prevent it and employ healthy hygiene. Drugs have serious side effects and cannot be used by the entire population and should not be used for long periods of time.
In order to control an epidemic all types of treatment should be employed including prescription drugs (ACE, ARB's, TNF-alpha blockers, anti-viral and anti-bacterial) vitamins, mineral, antioxidant herbs, proper hygiene, air filtration, water filtration and the proper use of diet and nutritional supplements, especially the newly patented, FDA approved Silver Sol technology. Silver Sol destroys bacteria, viruses, and mold so it demonstrates broader spectrum of activity than any antibiotic or antiviral drug. It can be taken daily due the fact that it passes through the body unchanged, and can prevent viral infections, treat them and work synergistically with antibiotics to produce as much as a ten fold increase in activity against the bacteria that cause death in influenza.
By Gordon Pedersen Ph.D.
Influenza viruses are the respiratory viruses of greatest public health importance, particularly Influenza A (1). Every year 36,000 people die from Influenza making it the 6th leading cause of death in America (1). The CDC estimates that it would cost America $71 – 166 billion if we have an Influenza epidemic today. Approximately 1 in every 1,000 swine flu patients dies from the infection. This is close to the same rate we have been seeing the past few years but antigenic drift and antigenic shift may create a new and fatal form of Influenza that humans have no immunity against (2). Antigenic drift is a variation within the HN sub-type. Antigenic shift is a variation between different HN sub-types, changes in the Heamagluttinin (H) and Neuraminiadase (N) makes large portions of the population immunologically naïve on a regular basis (1). The problem with Type A is that it undergoes both antigenic drift and antigenic shift making it more dangerous and unpredictable (1). The World Health Organization declared the H1N1 Swine Flu a pandemic in June of 2009 (3).
The annual average U.S. winter epidemics affect 5% to 20% of the population.
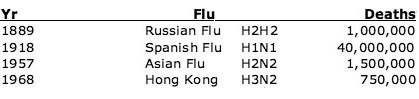
The CDC (1) reports the following pandemic death histories:
Health Care Practitioners Are At the Highest Risk
Doctors, nurses and other health care providers are at the highest risk of becoming infected with Influenza. Because doctors are exposed to the virus most frequently, it is significant to recognize the survivability of the Influenza virus in open environments.
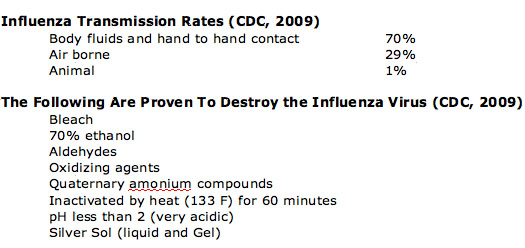
Mammalian Influenza A survives 1 hour in mucous, while Avian Influenza survives 100 days in water, 200 days @ 63 degrees F, 1 day in feces and indefinitely when frozen. Influenza is easily transmitted from human to human as indicated in the following table.
Doctors have the obligation to protect themselves and their patients from the potentially pandemic Influenza viruses. This protection could come from many different sources including Vaccination, Hygiene, Anti viral drugs, Antibiotic drugs, Nutritional supplements, Air filters, Water purifiers, Masks, Topical gels and Silver Sol.
Past epidemics provide important insights into what might happen in the potential spread of the current Swine Flu (4-13). The most persistent viruses survive and the most diverse seem to go extinct within a few years (14, 15). This is most likely the result of strong host-mediated selection pressure, resulting in continual evolution at key antigenic sites, a process termed ‘antigenic drift' (15, 16). This antigenic evolution is observed with major changes in antigenicity occurring periodically in patterns of approximately 3 years between episodes (17).
According to reports from the Army Medical records, (from the 1918 Spanish Flu, H1N1 epidemic) 24% of the people died from the virus and 76% died form a secondary bacterial infection that produced pneumonia in the lungs. There is a high probability that the swine flu will have similar death rates, and if this is the case, then preventing and treating the secondary bacterial infection will be as important if not more important. The conclusion is that the influenza virus will need to be treated by multiple or combination therapies crossing viral and bacterial lines.
Recommendations for Influenza prevention and treatment (1)
Hygiene: The CDC recommends washing the hands after any exposure because most influenza is transferred by hand contact. Masks and gloves can help but the mask must fit tightly with no leaks to be effective. A surgical mask helps protect the persons around the wearer, so if you have a fever, cough or sneeze, wear a surgical mask to protect the patients.
Anti viral drugs:
These drugs have the ability to destroy viruses but cannot be taken for an extended period of time. They produce side effects that mimic the flu making it difficult to diagnose the severity of the disease. If taken for prevention, Tamiflu produces resistance. 18% of the influenza virus is resistant to Tamiflu already (1). It is suspected that the health care professionals who were taking it for four months as a preventive agent were the persons that developed resistance. This indicates that we cannot use the antiviral drugs for long periods of time. In addition, some drugs cannot be used in children under 13 years of age (Tamiflu). Relenza cannot be used in children under one or in adults over 65. The antivirals must be given within 48 hours of the onset of illness or the virus will run its course. Combine this with the fact that 76% of H1N1 subjects in the Spanish flu 1918, died from a bacterial infection that produced pneumonia and you have an incomplete solution to the influenza problem. Because Tamiflu has developed resistance Relenza may be a better choice as long as you monitor the bronchospasms.
Antibiotic Drugs:
Antibiotic drugs provide no solution against the virus but can be very beneficial for pneumonia that develops later. A broad spectrum antibiotic should be used because there are numerous bacteria that can produce pneumonia. According to a Penn State publication, silver sol can be given with the antibiotics and produce up to a tenfold increase in antibiotic activity (18).
Nutritional Supplements:
There are hundreds of supplements that can be of significant benefit for the immune system and even some that claim to have antiviral activity. The best proven choices for nutritional supplements come in the form of immune stimulants and wellness products. These include: immunity Vit C, B complex, folic acid, vit D (prevention) ginseng, Echinacea, garlic, probiotics, expectorants and silver sol.
Air Filters:
CDC recommends one in every room. HEPA air filters use silver to inactivate viruses and can effectively kill 99% of all bacteria, and viruses in minutes.
Water Purifiers:
Proper hygiene and a water purifier are recommended by the CDC because the influenza virus can survive 100 hours in water. Get one that has a silver filter that can actually destroy the virus. Carbon, filtration, reverse osmosis does not destroy or remove the virus.
Topical Disinfectants:
Topical disinfectants are recommended by the CDC for use between each patient and can kill germs for 4-6 hours. Patients and health care professionals should use these 4 times a day or as needed. Silver so gel demonstrates effectiveness against some of the worst pathogens including: MRSA, VRE, Strep, and the other bacteria that cause pneumonia.
Silver Sol:
Prescription drugs and vaccines treat and help prevent viral infection and disease but are not capable of totally controlling a dangerous new or novel virus (18). Nutritional supplements such as Vitamins, Minerals, Echinacea, Ginseng, Probiotics and many others have the ability to help boost immune function and improve natural defenses which results in some defense against disease causing viruses and the associated secondary infections
Silver Sol provides proven prevention and treatment against viral and bacterial infections, while there is nothing else with such broad spectrum benefits (19). In addition, Silver Sol can be safely taken every day for prevention where it has been shown to provide protection against the very dangerous Bird flu H5N1. The combination of antibiotics with Silver Sol has been shown to enhance antibiotic function by as much as ten fold due to the fact that Silver Sol kills the residual pathogens that the antibiotics cannot (19). Results of the combination of 19 different prescription antibiotics and silver sol demonstrate safe additive and/or synergistic benefits across 7 different pathogenic strains (Staphyloccocus, MRSA, E coli, Pseudomonas arugenosa, Salmonella and Streptococcus). The results of this combination therapy result in significant pathogenic destruction while helping to reduce bacterial resistance (19). This can be attributed to the fact that Silver Sol does not produce resistance, nor does it destroy the benefitcial intestinal probiotic bacteria (18).
Discussion:
H1N1 is a serious threat to our health and way of life. The best way to treat it influenza is to prevent it. Prevention produces a problem is that drugs have serious side effects and cannot be used by the entire population and should not be used for long periods of time. The other problem is that approximately three fourths of the people who have died from H1N1 influenza have succumbed to a secondary bacterial infection in the lungs and no antiviral drug will treat this condition.
In order to control an epidemic, all types of treatment should be employed including prescription drugs, vitamins, mineral, herbs, proper hygiene, air filtration, water filtration and the proper use of diet and nutritional supplements, especially the newly patented, FDA approved Silver Sol technology. Silver Sol destroys bacteria, viruses, and mold so it demonstrates broader spectrum of activity than any antibiotic or antiviral drug. It can be taken daily due the fact that it passes through the body unchanged, and can prevent viral infections, treat them and work synergistically with antibiotics to produce as much as a ten fold increase in activity against the bacteria that cause death in influenza. It is evident that the newly patented EPA certified and FDA approved Silver Sol technology provides tremendous treatment options for prevention and combination therapies. Silver Sol gel can help stop viral spread on the most contagious areas like hands, nose, mouth and skin. It is sufficiently documented and proven to be considered to be a first line of defense against Influenza and a significant companion to antiviral and antibacterial drug regimens topically and orally.
References
1. Centers for Disease Control contributing Authors: Burke Squires (UTSW), Marc Gillespie (CSHL), Peter E'dustacio (CSHL), Adolfo Garc�a-Sastre (MSSM).
2. CDC. Update: swine-origin influenza A (H1N1) virus---United States and other countries. MMWR 2009;58:421.
3. Novel Swine-Origin Influenza A (H1N1) Virus Investigation Team. Emergence of a novel swine-origin influenza A (H1N1) virus in humans. N Engl J Med 2009;361.
4. World Health Organization. Situation updates---influenza A (H1N1). Geneva, Switzerland: World Health Organization; 2009.
5. Rowe T, Abernathy RA, Hu-Primmer J, et al. Detection of antibody to avian influenza A (H5N1) virus in human serum by using a combination of serologic assays. J Clin Microbiol 1999;37:937--43.
6. Laver WG, Webster RG. Selection of antigenic mutants of influenza viruses. Isolation and peptide mapping of their hemagglutination proteins. Virology. 1968;34:193–202.
7. Sleigh MJ, Both GW, Underwood PA, Bender VJ. Antigenic drift in the hemagglutinin of the Hong Kong influenza subtype: correlation of amino acid changes with alterations in viral antigenicity. J Virol. 1981;37:845–853.
8. Fitch WM, Leiter JMF, Li X, Palese P. Positive Darwinian evolution in human influenza A viruses. Proc Natl Acad Sci. 1991;88:4270–4272.
9. Bush RM, Fitch WM, Bender CA, Cox NJ. Positive selection on the H3 hemagglutinin gene of human influenza virus A. Mol Biol Evol. 1999;16:1457–1465.
10. Rvachev LA. Computer modeling experiment on large-scale epidemic. Dokl USSR Acad Sci. 1968;2:294–296.
11. Longini IM, Fine PE, Thacker SB. Predicting the global spread of new infectious agents. Am J Epidemiol. 1986;123:383–391.
12. Bonabeau E, Toubiana L, Flahault A. The geographical spread of influenza. Proc Biol Sci. 1998;265:2421–2425.
13. Grais RF, Ellis JH, Glass GE. Assessing the impact of airline travel on the geographic spread of pandemic influenza. Eur J Epidemiol. 2003;19:1065–1072.
14. Viboud C, Bjørnstad ON, Smith DL, Simonsen L, Miller MA, et al. Synchrony, waves, and spatial hierarchies in the spread of influenza. Science. 2006;312:447–451.
15. Buonagurio DA, Nakada S, Parvin JD, Krystal M, Palese P, Fitch WM. Evolution of human influenza A viruses over 50 years: rapid, uniform rate of change in NS gene. Science. 1986;232:980–982.
16. Fitch WM, Leiter JMF, Li X, Palese P. Positive Darwinian evolution in human influenza A viruses. Proc Natl Acad Sci. 1991;88:4270–4272.
17. Fitch WM, Bush RM, Bender CA, Cox NJ. Long term trends in the evolution of H(3) HA1 human influenza type A. Proc Natl Acad Sci. 1997;94:7712–7128.
18. Smith DJ, Lapedes AS, de Jong JC, Bestebroer TM, Rimmelzwaan GF, Osterhaus AD, Fouchier RA. Mapping the antigenic and genetic evolution of influenza virus. Science. 2004;305:371–376.
19. Ferguson NM, Galvani AP, Bush RM. Ecological and immunological determinants of influenza evolution. Nature. 2003;422:428–433.
20. Thompson WW, Shay DC, Weintraub E, Brammer L, Cox N, et al. Mortality associated with influenza and respiratory syncytial virus in the United States. JAMA. 2003;289:179–186.
21. Thompson WW, Shay DC, Weintraub E, Brammer L, Bridges CB, et al. Influenza- Associated hospitalizations in the United States. JAMA. 2004;292:1333–1340.
22. Ina Y, Gojobori N. Statistical analysis of nucleotide sequences of the hemagglutinin gene of human influenza A viruses. Proc Natl Acad Sci. 1994;91:8388–8392.
23. Hay AJ, Gregory V, Douglas AR, Lin YP. The evolution of human influenza viruses. Phil Trans R Soc Lond B. 2001;356:1861–1870.
24. Jenkins GM, Rambaut A, Pybus OG, Holmes EC. Rates of molecular evolution in NA viruses: a quantitative phylogenetic analysis. 2002;54:156–165.
25. Centers for Disease Control and Prevention. Update: influenza activity–United States and worldwide, 2006-2007 and composition of the 2007–2008 influenza vaccine. MMWR. 2007;56:789–794.
26. Roy, R. Ultradilute Material Research Innovations, Ag-aquasols with extradrdinary bactericidal properties: role of the system Ag-O-H2O. 2007 vol 11 no 1.
27. Pedersen, G., Effect of Prophylactic Treatment with ASAP – AGX-32 and nd ASAP Solutions on an Avian Influenza A (H5N1) Virus Infecrion in Mice.
28 Nelson Labs . Hepatitis B and Silver Sol.
29. De Souza. A., Mehta, D, Bactericidal activity of Combinations of Silver-Water Dispersion with 19 Antibiotics Against Seven Microbial Strains. Current Science, Vol 91, No 7, October 2006.
30. Leavitt, R, Pedersen G,. Resistance of Silver Sol and Bacteria: A Discussion, ABL, 2009.
31 Viridis BioPharma, Probiotic Bacteria and Silver Sol, 2007.
32. Laver WG, Webster RG. Selection of antigenic mutants of influenza viruses. Isolation and peptide mapping of their hemagglutination proteins. Virology. 1968;34:193–202.
33. Sleigh MJ, Both GW, Underwood PA, Bender VJ. Antigenic drift in the hemagglutinin of the Hong Kong influenza subtype: correlation of amino acid changes with alterations in viral antigenicity. J Virol. 1981;37:845–853.
34. Fitch WM, Leiter JMF, Li X, Palese P. Positive Darwinian evolution in human influenza A viruses. Proc Natl Acad Sci. 1991;88:4270–4272.
35. Bush RM, Fitch WM, Bender CA, Cox NJ. Positive selection on the H3 hemagglutinin gene of human influenza virus A. Mol Biol Evol. 1999;16:1457–1465.
36. Rvachev LA. Computer modeling experiment on large-scale epidemic. Dokl USSR Acad Sci. 1968;2:294–296.
37. Longini IM, Fine PE, Thacker SB. Predicting the global spread of new infectious agents. Am J Epidemiol. 1986;123:383–391.
38. Bonabeau E, Toubiana L, Flahault A. The geographical spread of influenza. Proc Biol Sci. 1998;265:2421–2425.
39. Grais RF, Ellis JH, Glass GE. Assessing the impact of airline travel on the geographic spread of pandemic influenza. Eur J Epidemiol. 2003;19:1065–1072.
40. Viboud C, Bjørnstad ON, Smith DL, Simonsen L, Miller MA, et al. Synchrony, waves, and spatial hierarchies in the spread of influenza. Science. 2006;312:447–451.
41. Buonagurio DA, Nakada S, Parvin JD, Krystal M, Palese P, Fitch WM. Evolution of human influenza A viruses over 50 years: rapid, uniform rate of change in NS gene. Science. 1986;232:980–982.
42. Fitch WM, Leiter JMF, Li X, Palese P. Positive Darwinian evolution in human influenza A viruses. Proc Natl Acad Sci. 1991;88:4270–4272.
43. Fitch WM, Bush RM, Bender CA, Cox NJ. Long term trends in the evolution of H(3) HA1 human influenza type A. Proc Natl Acad Sci. 1997;94:7712–7128.
44. Smith DJ, Lapedes AS, de Jong JC, Bestebroer TM, Rimmelzwaan GF, Osterhaus AD, Fouchier RA. Mapping the antigenic and genetic evolution of influenza virus. Science. 2004;305:371–376.
45. Ferguson NM, Galvani AP, Bush RM. Ecological and immunological determinants of influenza evolution. Nature. 2003;422:428–433.
6. Koelle K, Cobey S, Grenfell B, Pascual M. Epochal evolution shapes the phylodynamics of interpandemic influenza A (H3N2) in humans. Science. 2006;314:1898–903.
47. Rambaut A, Pybus O, Nelson MI, Viboud C, Taubenberger JK, et al. The genomic and epidemiological dynamics of human influenza A virus. Nature April 16; [Epub ahead of print]
48. Lavenu A, Leruez-Ville M, Chaix ML, Boelle PY, Rogez S, Freymuth F, Hay A, Rouzioux C, Carrat F. Detailed analysis of the genetic evolution of influenza virus during the course of an epidemic. Epidemiol Infect. 2005:1–7.
49. Nelson MI, Simonsen L, Viboud C, Miller MA, Taylor J, et al. Stochastic processes are key determinants of the short-term evolution of influenza A virus. PLoS Pathog. 2006;2:e125. doi:10.1371/journal.ppat.0020125.
50. Viboud C, Alonso WJ, Simonsen L. Influenza in tropical regions. PLoS Med. 2006;3:e89. doi:10.1371/journal.pmed.0030089.
51. Nelson MI, Simonsen L, Viboud C, Miller MA, Holmes EC. Phylogenetic analysis reveals the global migration of seasonal influenza A viruses. PLoS Pathog. 2007;3:e131. doi:10.1371/journal.ppat.0030131.
52. Russell CA, Jones TC, Barr IG, Cox NJ, Garten RJ, et al. The global circulation of seasonal influenza A (H3N2) viruses. Science. 2008;320:340–346.
53. Holmes EC, Ghedin E, Miller N, Taylor J, Bao Y, et al. Whole-genome analysis of human influenza A virus reveals multiple persistent lineages and reassortment among recent H3N2 viruses. PLoS Biol. 2005;3:e300. doi:10.1371/journal.pbio.0030300.
54. Nelson MI, Viboud C, Simonsen L, Bennett RT, Griesemer SB, et al. Multiple reassortment events in the evolutionary history of A/H1N1 influenza A virus since 1918. PLoS Pathog. 2008;4:e1000012. doi:10.1371/journal.ppat.1000012.
55. Nelson MI, Holmes EC. The evolution of epidemic influenza. Nat Rev Genet. 2007;8:196–205.
56. Thompson WW, Shay DC, Weintraub E, Brammer L, Cox N, et al. Mortality associated with influenza and respiratory syncytial virus in the United States. JAMA. 2003;289:179–186.
57. Thompson WW, Shay DC, Weintraub E, Brammer L, Bridges CB, et al. Influenza-associated hospitalizations in the United States. JAMA. 2004;292:1333–1340.
58. Ina Y, Gojobori N. Statistical analysis of nucleotide sequences of the hemagglutinin gene of human influenza A viruses. Proc Natl Acad Sci. 1994;91:8388–8392.
59. Hay AJ, Gregory V, Douglas AR, Lin YP. The evolution of human influenza viruses. Phil Trans R Soc Lond B. 2001;356:1861–1870.
60. Jenkins GM, Rambaut A, Pybus OG, Holmes EC. Rates of molecular evolution in NA viruses: a quantitative phylogenetic analysis. 2002;54:156–165.
61. Centers for Disease Control and Prevention. Update: influenza activity–United States and worldwide, 2006-2007 and composition of the 2007–2008 influenza vaccine. MMWR. 2007;56:789–794.
62. Simonsen L, Reichert TA, Viboud C, Blackwelder WC, Taylor RJ, et al. Impact of influenza vaccination on seasonal mortality in the US elderly population. Arch Intern Med. 2005;165:265–272.
63 a b Osterholm, Michael T. (2005-05-05). "Preparing for the Next Pandemic". The New England Journal of Medicine 352 (18): 1839–1842. doi:10.1056/NEJMp058068. PMID 15872196.
64 a b c Drazen, Jeffrey M.; Cecil, Russell L.; Goldman, Lee; Bennett, J. Claude (2000). Cecil Textbook of Medicine (21st ed.). Philadelphia: W.B. Saunders.
65. Thelancetoncology, (February 2007). "Leading Edge: High stakes, high risks". Lancet Oncology (The Lancet) 8 (2): 85. doi:10.1016/S1470-2045(07)70004-9. PMID 17267317.
66 Coghlan A (2006-08-14). "Mystery over drug trial debacle deepens". Health. New Scientist.
67 Ferrara, JL.; S. Abhyankar, DG. Gilliland (February 1993). "Cytokine storm of graft-versus-host disease: a critical effector role for interleukin-1". Transplant Proc. 2 (25): 1216–1217. PMID 8442093.
68 Huang KJ, Su IJ, Theron M, Wu YC, Lai SK, Liu CC, Lei HY (February 2005). "An interferon-gamma-related cytokine storm in SARS patients". Journal of Medical Virology 75 (2): 185–94. doi:10.1002/jmv.20255. PMID 15602737.
69 Haque A, Hober D, Kasper LH (October 2007). "Confronting potential influenza A (H5N1) pandemic with better vaccines". Emerging Infectious Diseases 13 (10): 1512–8. PMID 18258000.
70 Lacey M McNeil DG Jr (2009-04-24). "Fighting Deadly Flu, Mexico Shuts Schools". NYTimes.com.
71 a b "Interim Guidance for Clinicians on Identifying and Caring for Patients with Swine-origin Influenza A (H1N1) Virus Infection". Centers for Disease Control and Prevention (CDC). 2009-04-29.
72 a b Humphreys, IR; G Walzl, L Edwards, A Rae, S Hill, T Hussell (2003-10-20). "A critical role for OX40 in T cell-mediated immunopathology during lung viral infection". J Exp Med. 198 (8): 1237–1242. doi:10.1084/jem.20030351. PMID 14568982.
73 Bhattacharya S (2003-10-20). "New flu drug calms the 'storm'". New Scientist.
74 OX-40 Clinical Trial details,
75 Genctoy, G; B Altun et al. (February 2005). "TNF alpha-308 genotype and renin-angiotensin system in hemodialysis patients: an effect on inflammatory cytokine levels?". Artif Organs 29 (2): 174–178. doi:10.1111/j.1525-1594.2005.29029.x. PMID 15670287.
76 Moldobaeva, A; EM Wagner (December 2003). "Angiotensin-converting enzyme activity in ovine bronchial vasculature". J Appl Physiol (Department of Medicine, Johns Hopkins University) 95 (6): 2278–2284. doi:10.1152/japplphysiol.00266.2003 (inactive 2009-04-29). PMID 15670287.
77 Shigehara, K; N Shijubo et al. (April 2003). "Increased circulating interleukin-12 (IL-12) p40 in pulmonary sarcoidosis". Clin Exp Immunol (Sapporo Medical University School of Medicine) 132 (1): 152–157. doi:10.1046/j.1365-2249.2003.02105.x. PMID 12653850.
78 Marshall, RP; P Gohlke et al. (January 2004). "Angiotensin II and the fibroproliferative response to acute lung injury". Am J Physiol Lung Cell Mol Physiol (Royal Free and University College London Medical School) 286 (1): 156–164. doi:10.1152/ajplung.00313.2002. PMID 12754187.
79 Wang, R; G Alam et al. (November 2000). "Apoptosis of lung epithelial cells in response to TNF-alpha requires angiotensin II generation de novo". J Cell Physiol (The Cardiovascular Institute, Michael Reese Hospital and Medical Center) 185 (2): 253–259. doi:10.1002/1097-4652(200011)185:2<253::AID-JCP10>3.0.CO;2-#. PMID 11025447.
80 Das UN (May 2005). "Angiotensin-II behaves as an endogenous pro-inflammatory molecule". The Journal of the Association of Physicians of India 53: 472–6. PMID 16124358.
81 Gelinck LB, van der Bijl AE, Beyer WE, Visser LG, Huizinga TW, van Hogezand RA, Rimmelzwaan GF, Kroon FP (May 2008). "The effect of anti-tumour necrosis factor alpha treatment on the antibody response to influenza vaccination". Annals of the Rheumatic Diseases 67 (5): 713–6. doi:10.1136/ard.2007.077552. PMID 17965123.






